Case 01
Severe Lumbar Spinal Stenosis Treated With Biportal Endoscopic Decompression
Biportal Decompression for Severe Lumbar Stenosis
- Diagnosis
- Severe lumbar spinal stenosis with radicular symptoms and objective neurologic deficit.
- Procedure
- Biportal endoscopic lumbar decompression.
- Surgical level
- Clinically concordant lumbar stenosis level or levels.
- Clinical presentation
- The patient presented with persistent leg-dominant symptoms despite medication, physical therapy, and injection treatment. The clinical findings included left-sided sensory disturbance in an L5 dermatome distribution and motor weakness involving ankle dorsiflexion and great toe dorsiflexion.
- Neurologic findings
- Preoperative neurologic examination demonstrated left ankle dorsiflexion weakness, approximately grade 3, and left great toe dorsiflexion weakness, approximately grade 3. Sensory disturbance was documented in the left L5 dermatome. These findings were reviewed together with imaging before surgical planning.
- Conservative treatment summary
- The patient had persistent symptoms despite medication, physical therapy, and injection treatment. Surgical treatment was considered because symptoms and neurologic findings persisted and were concordant with the stenotic level.
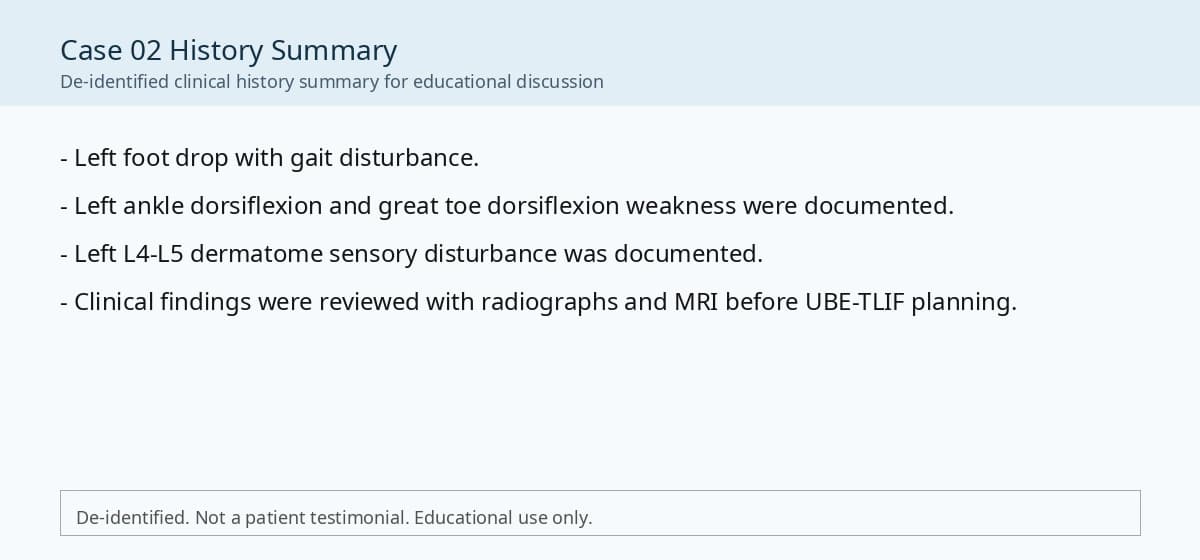
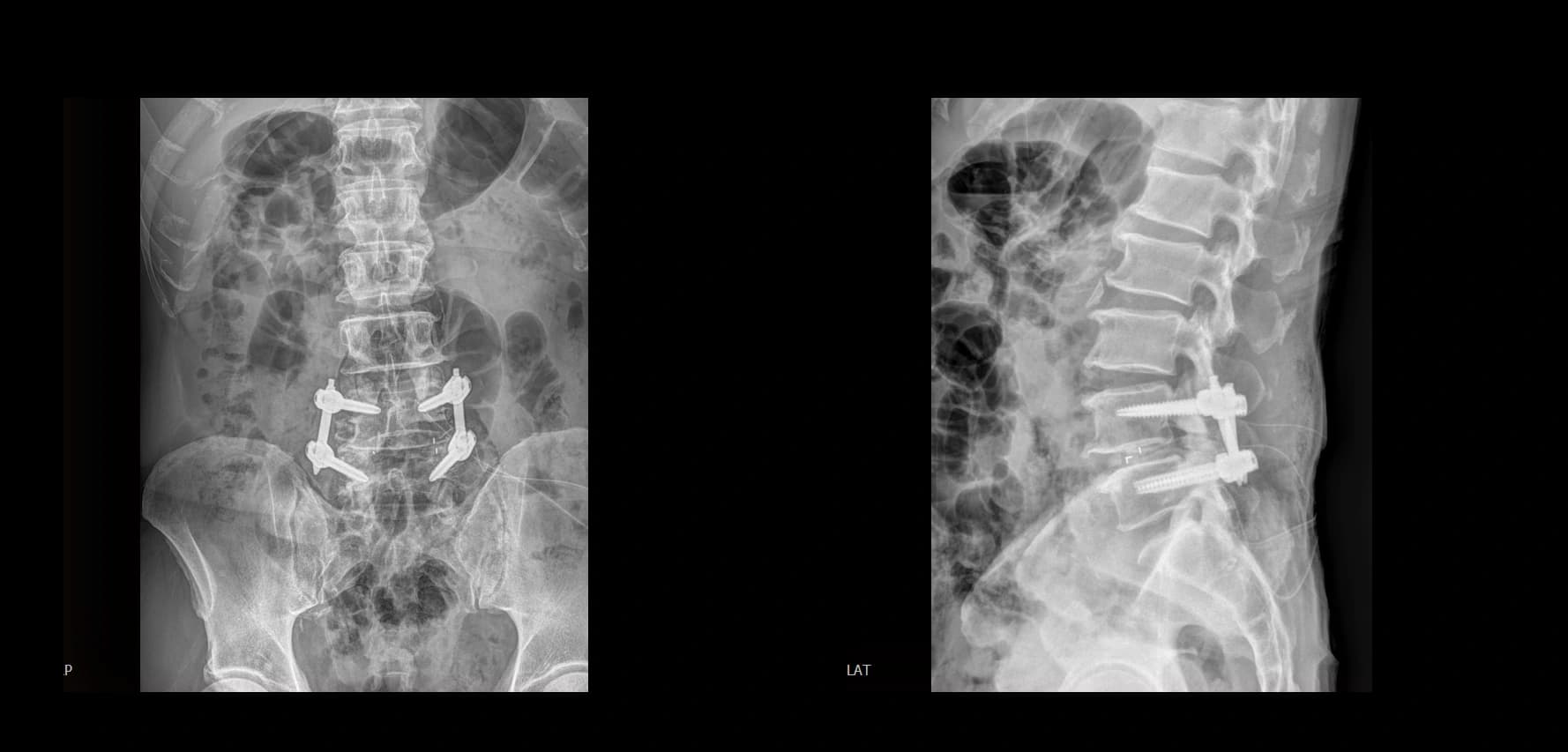
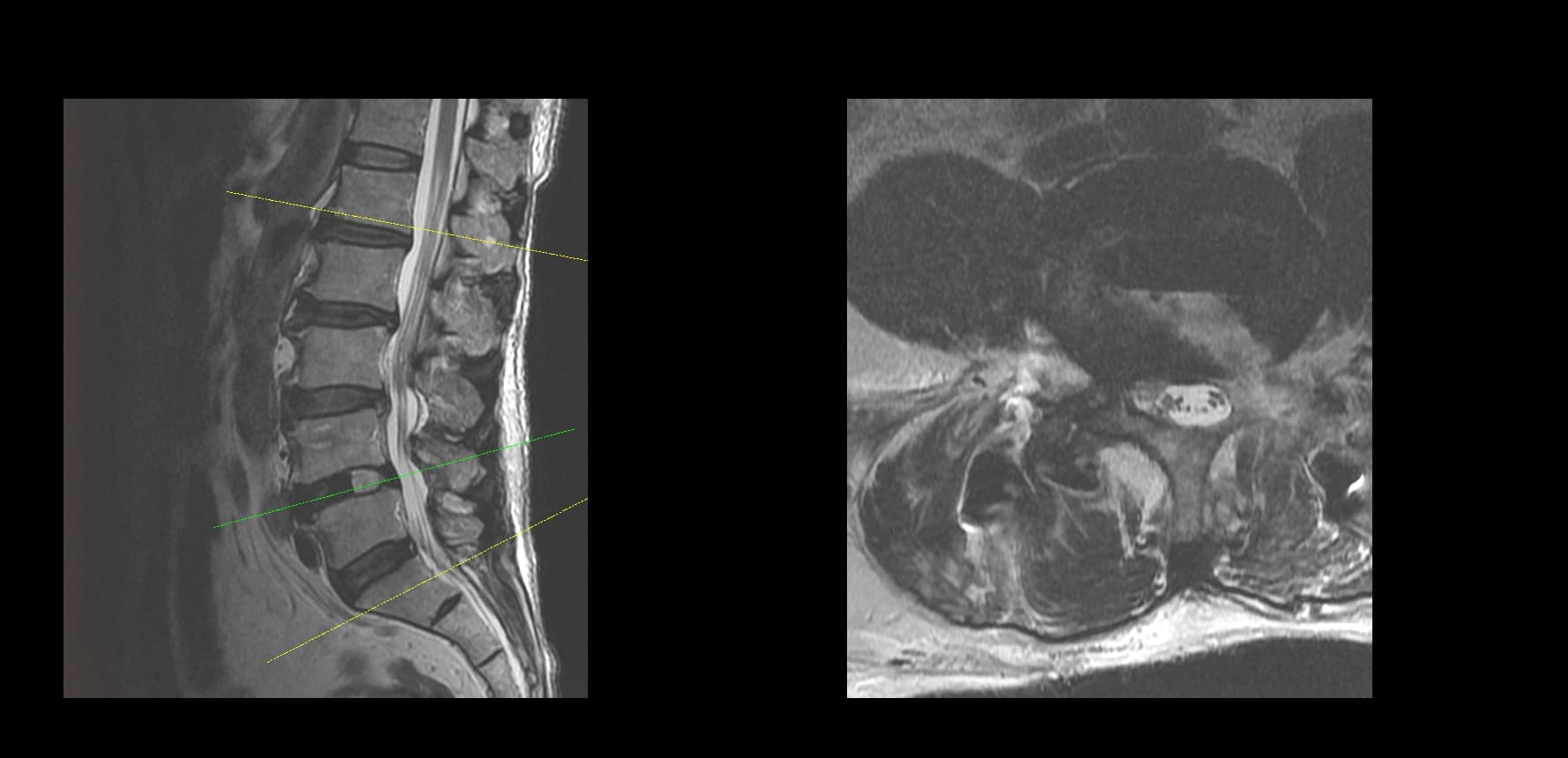
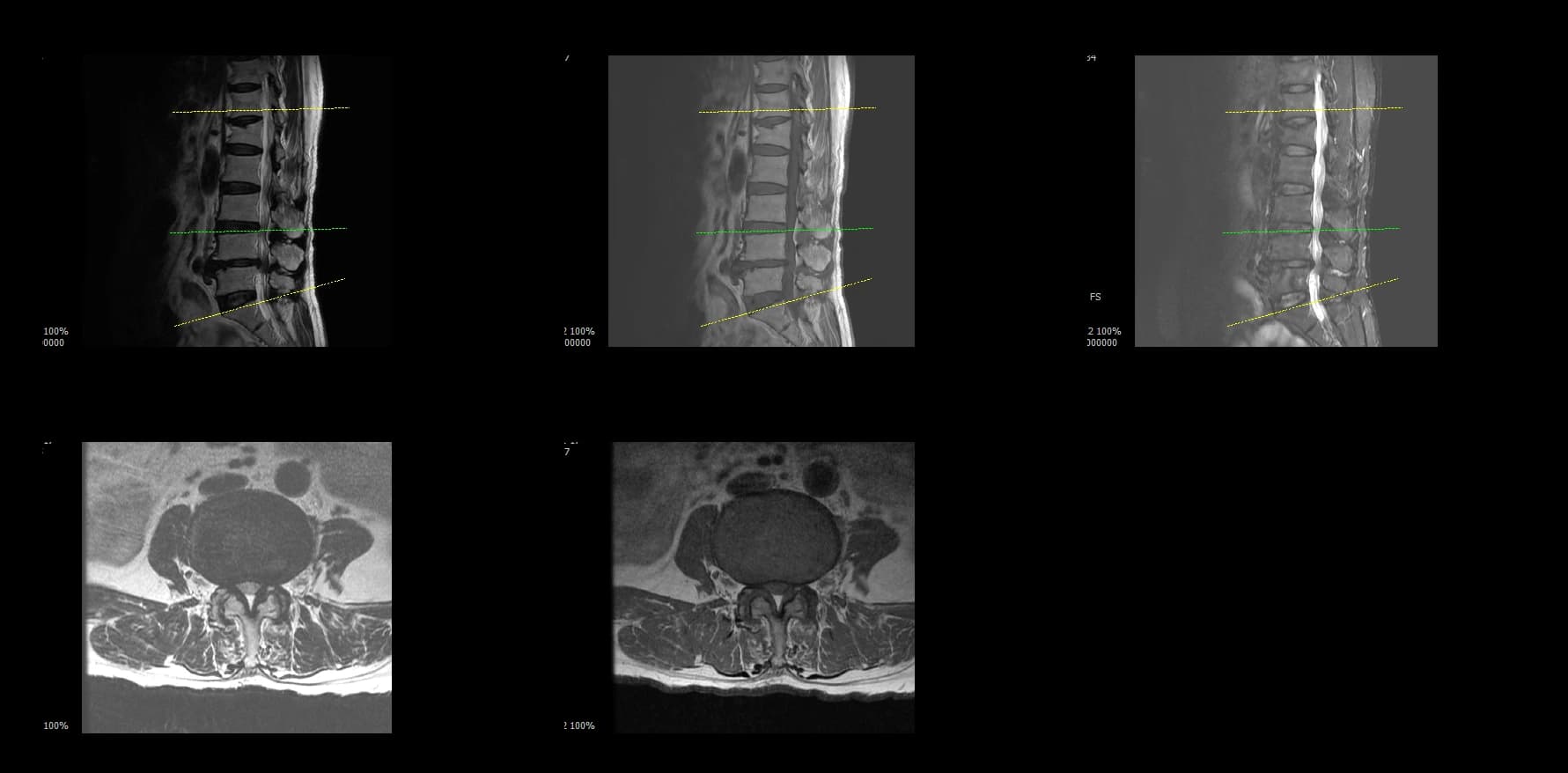
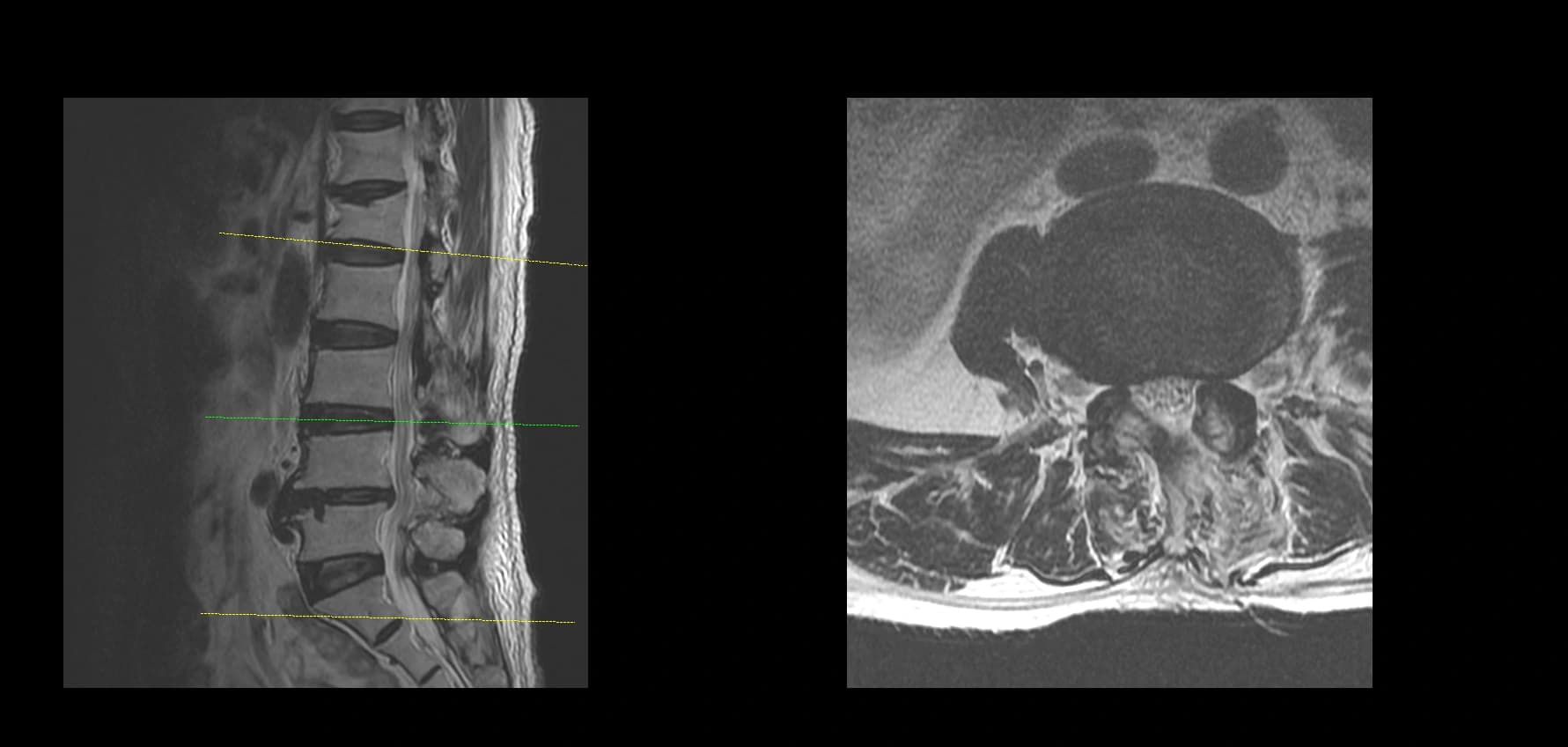
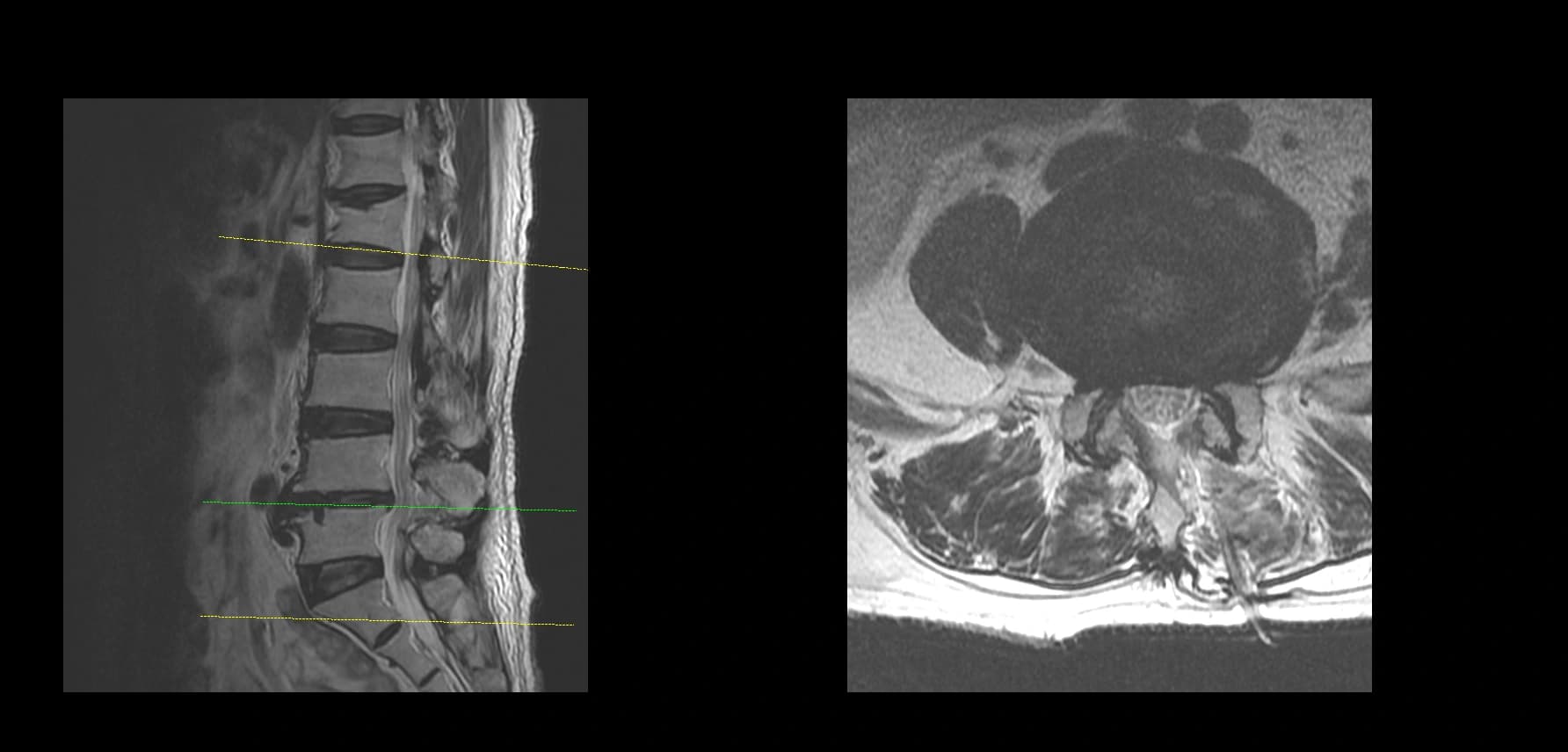
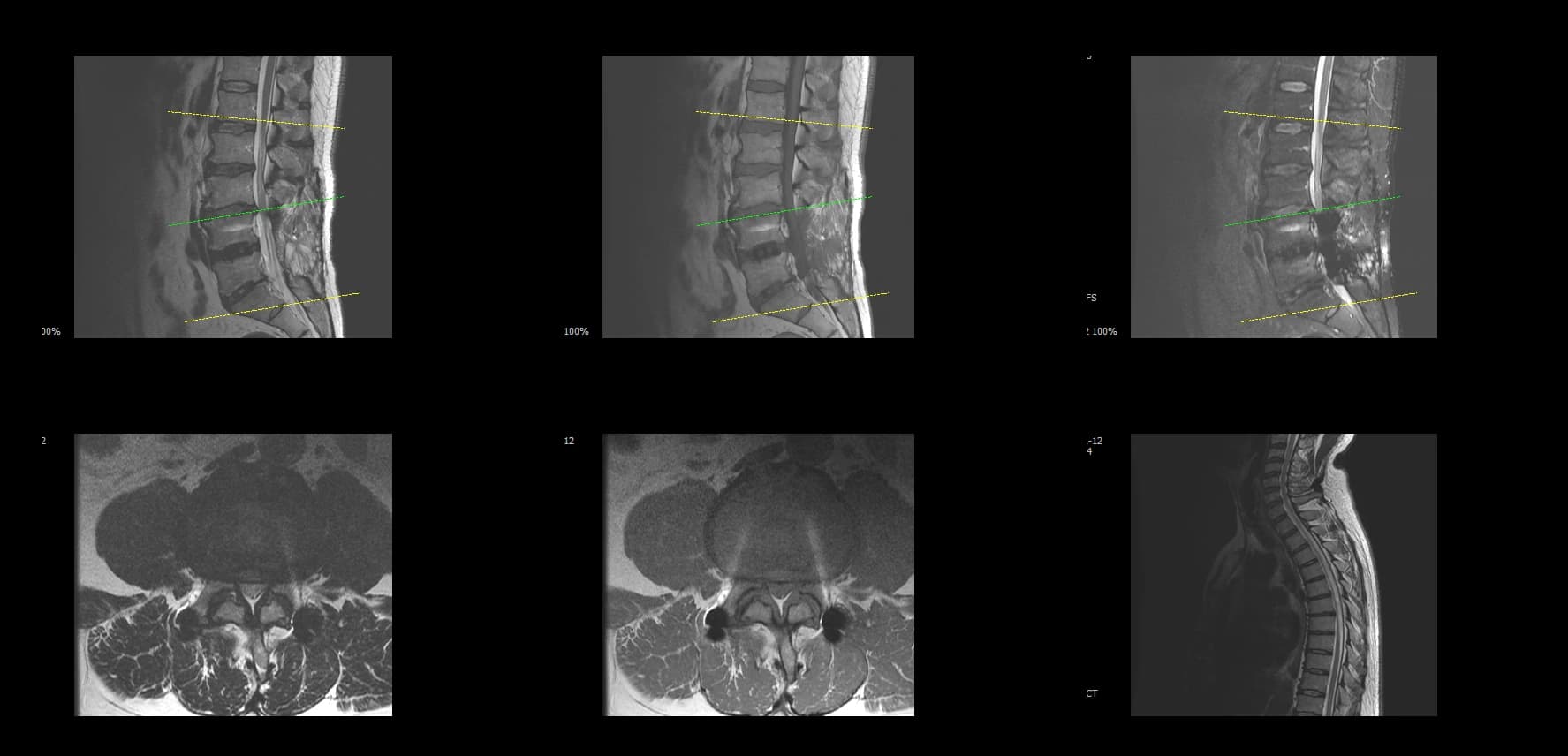
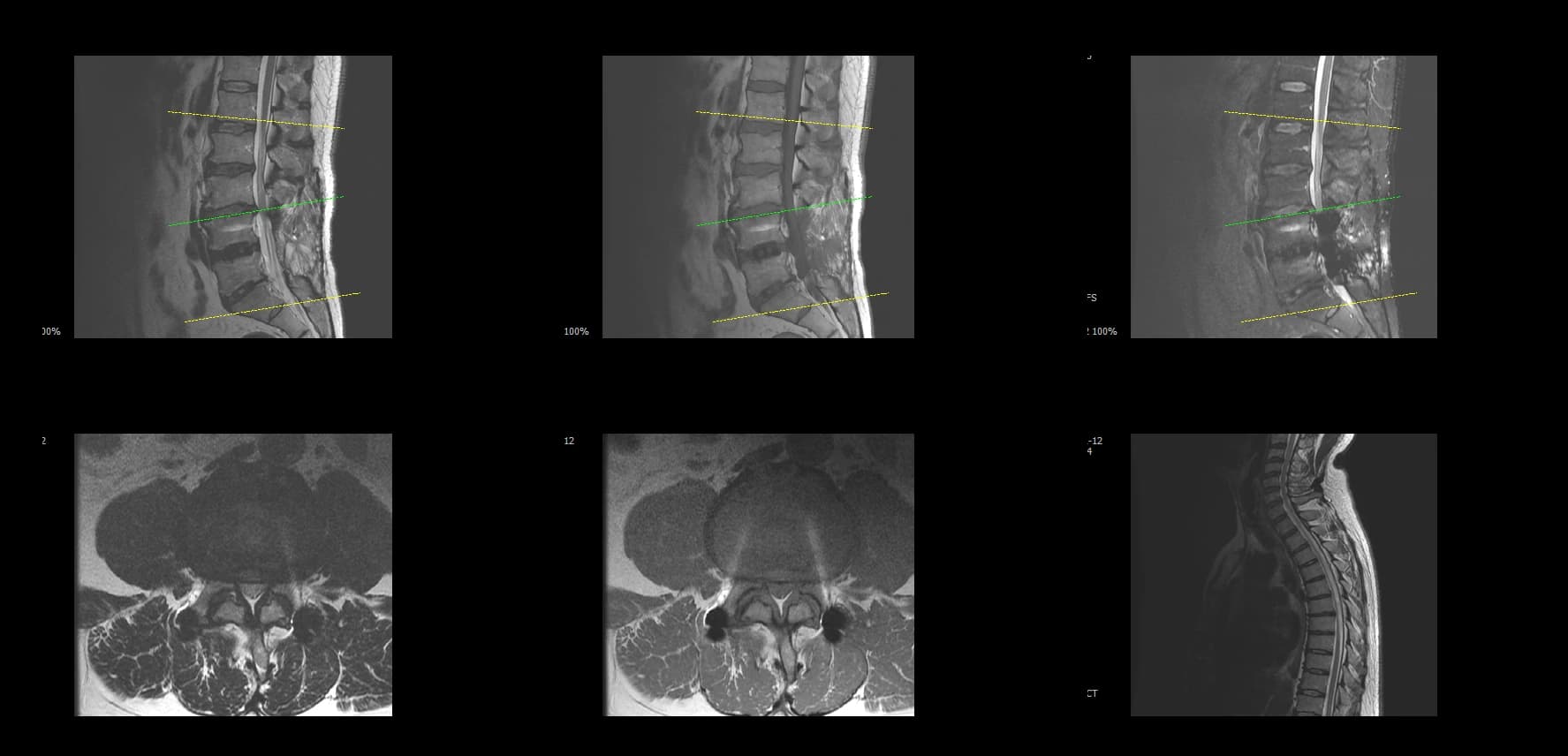
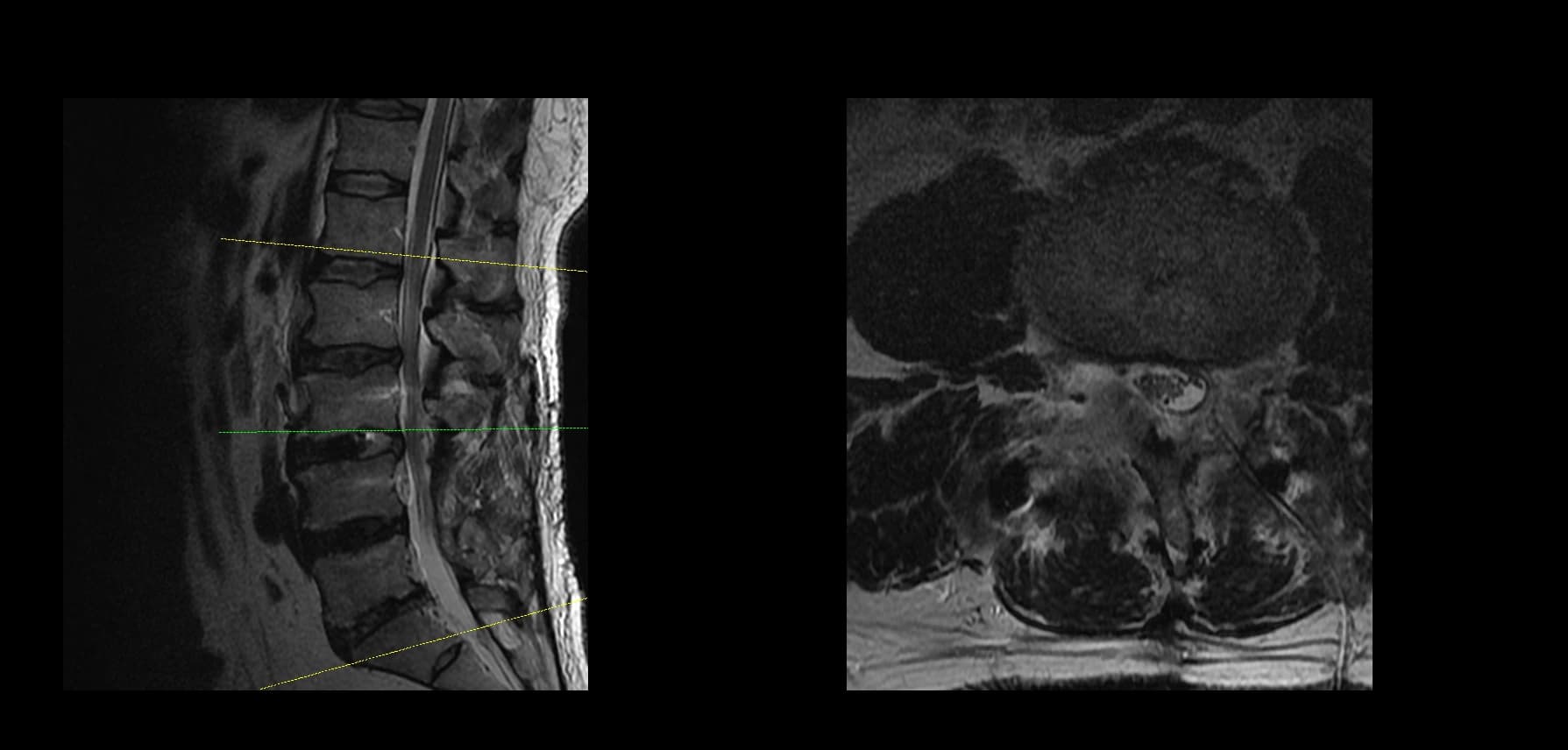
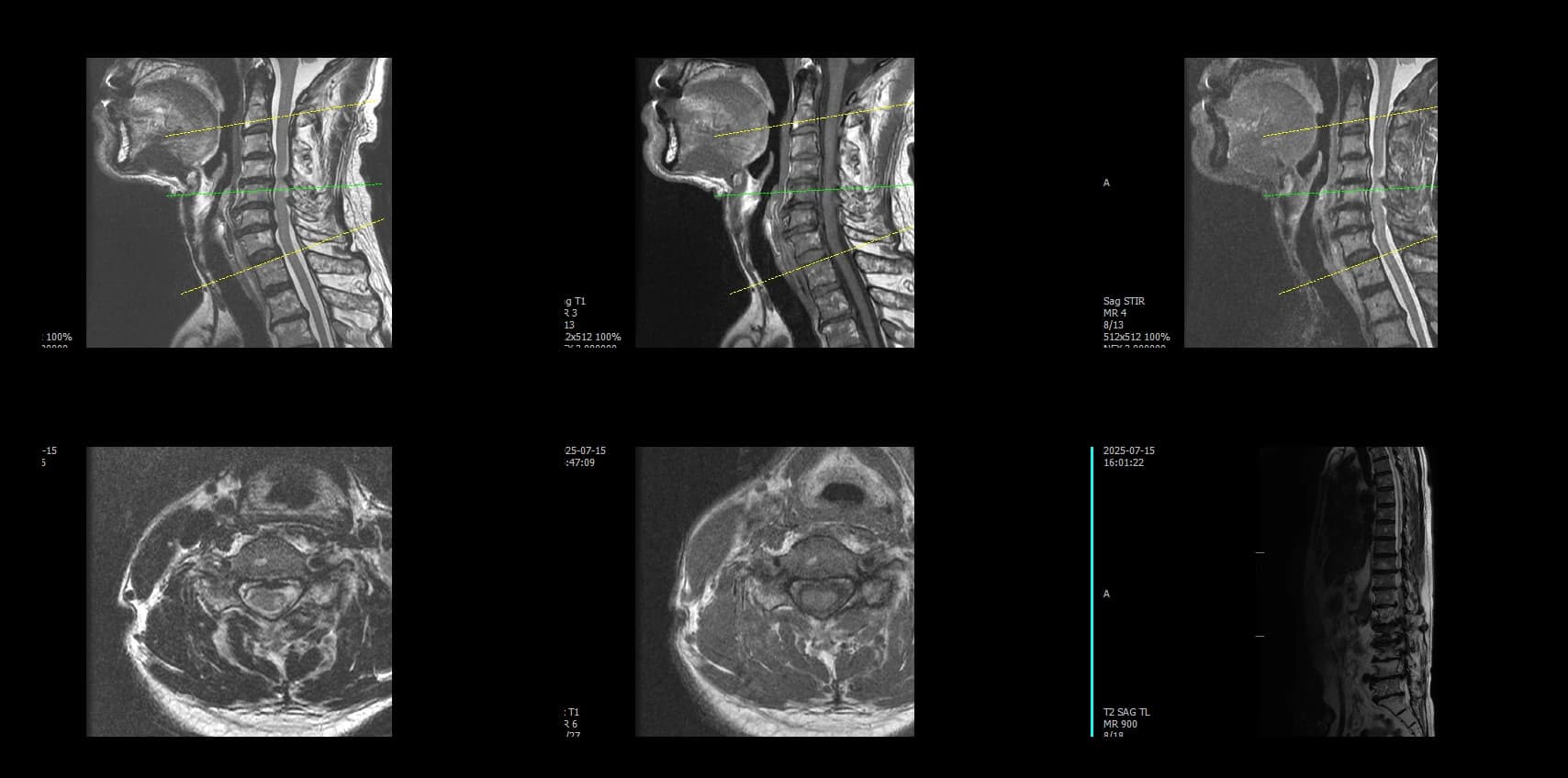
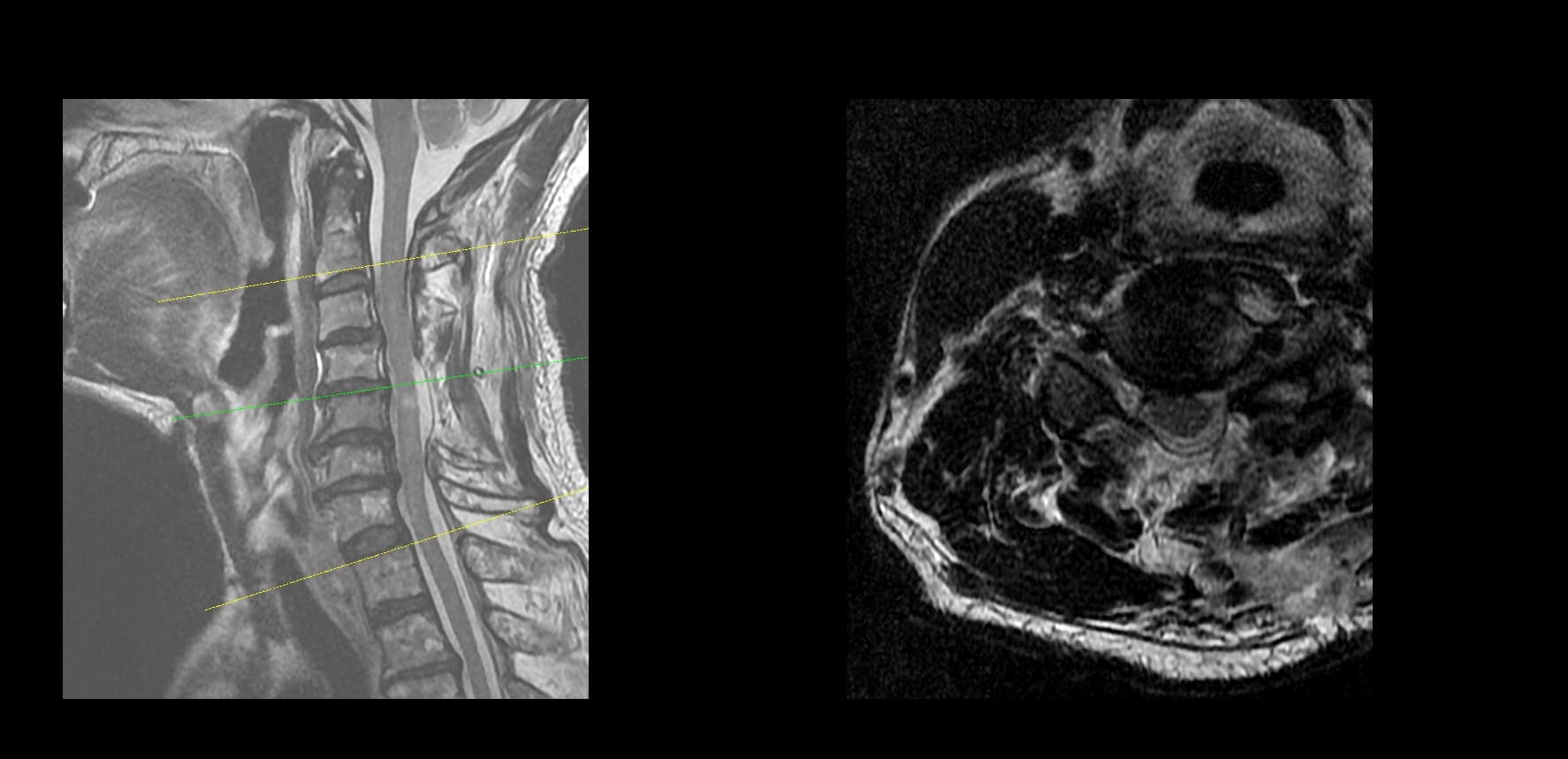
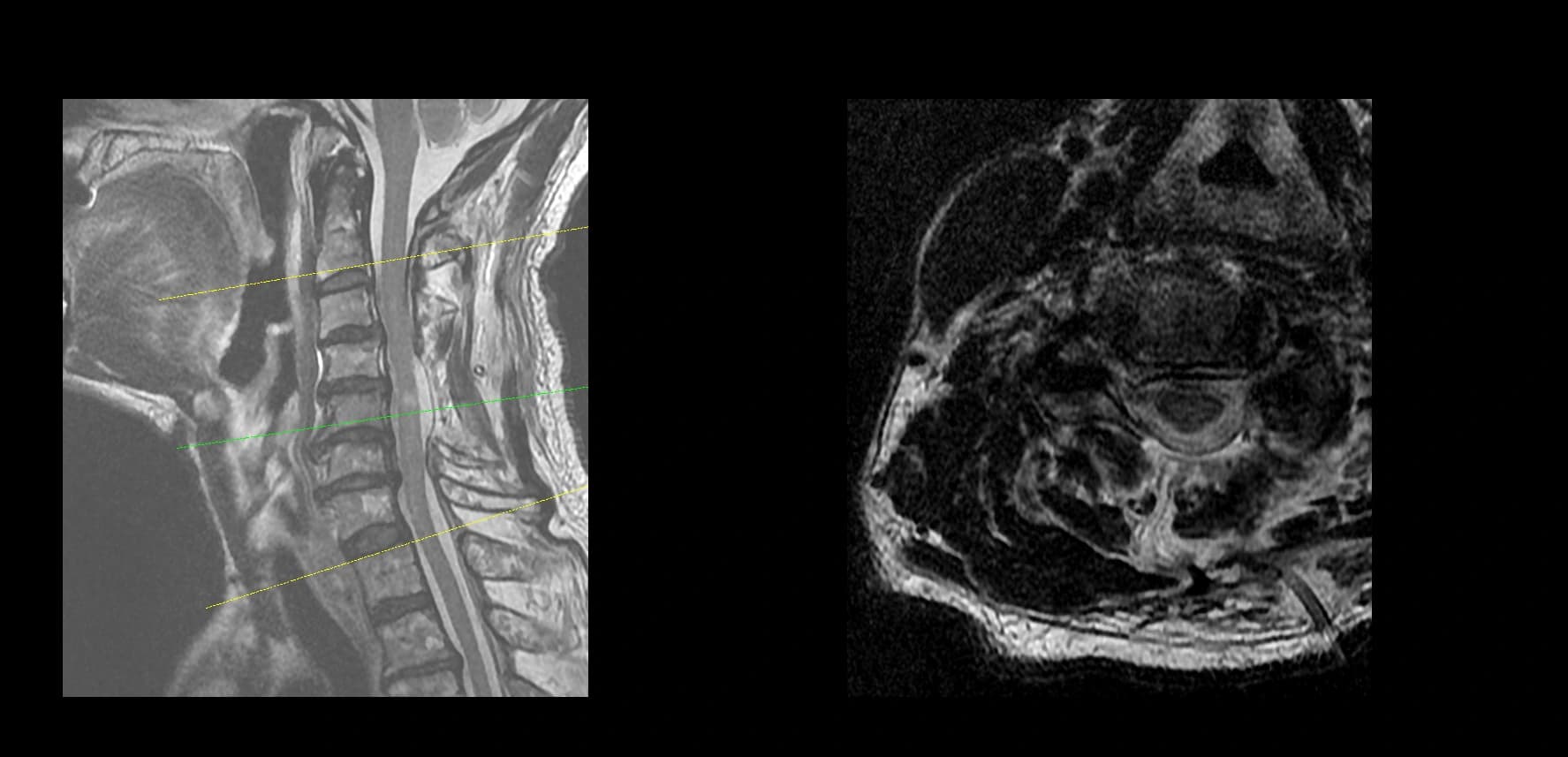
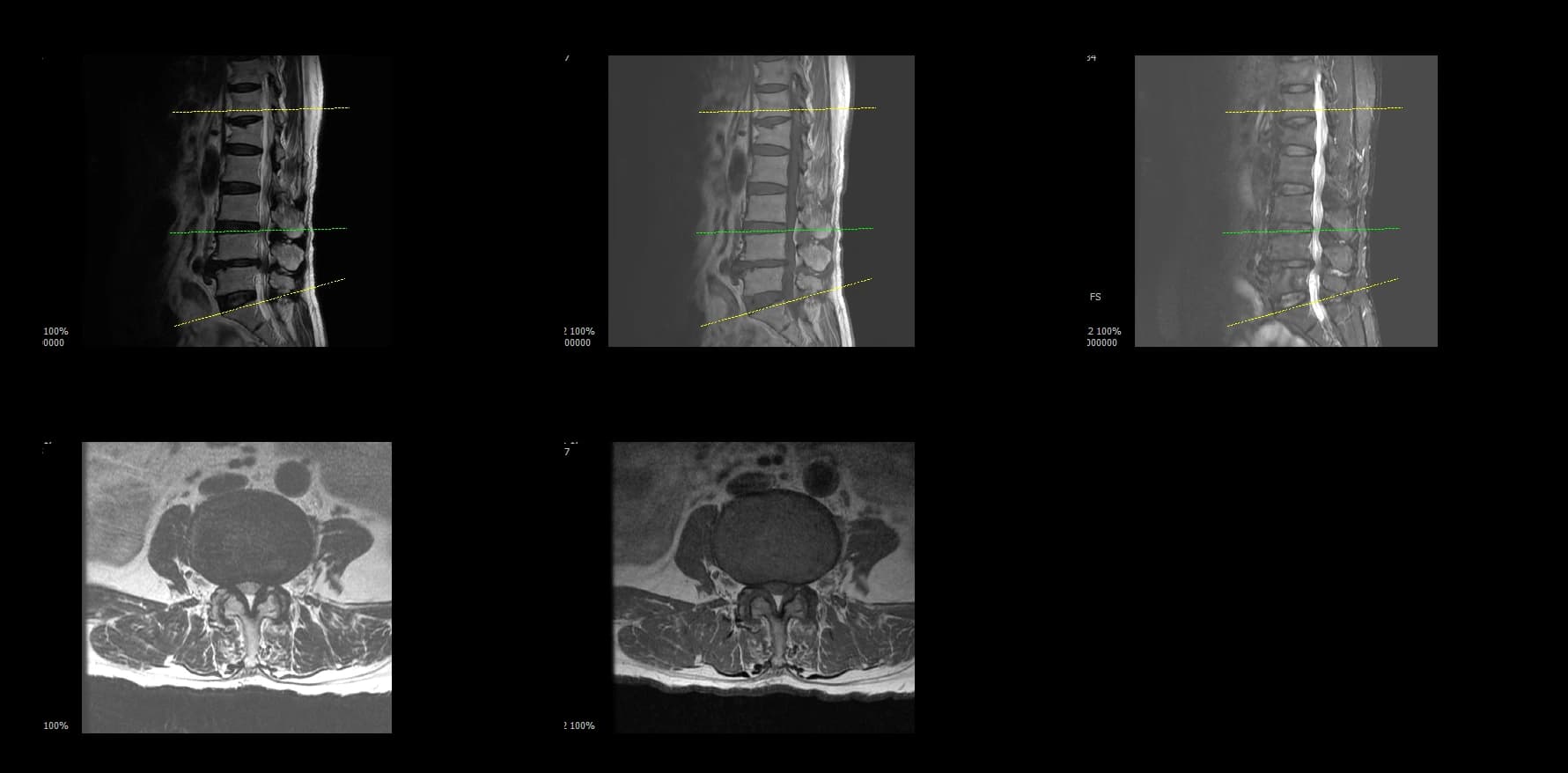
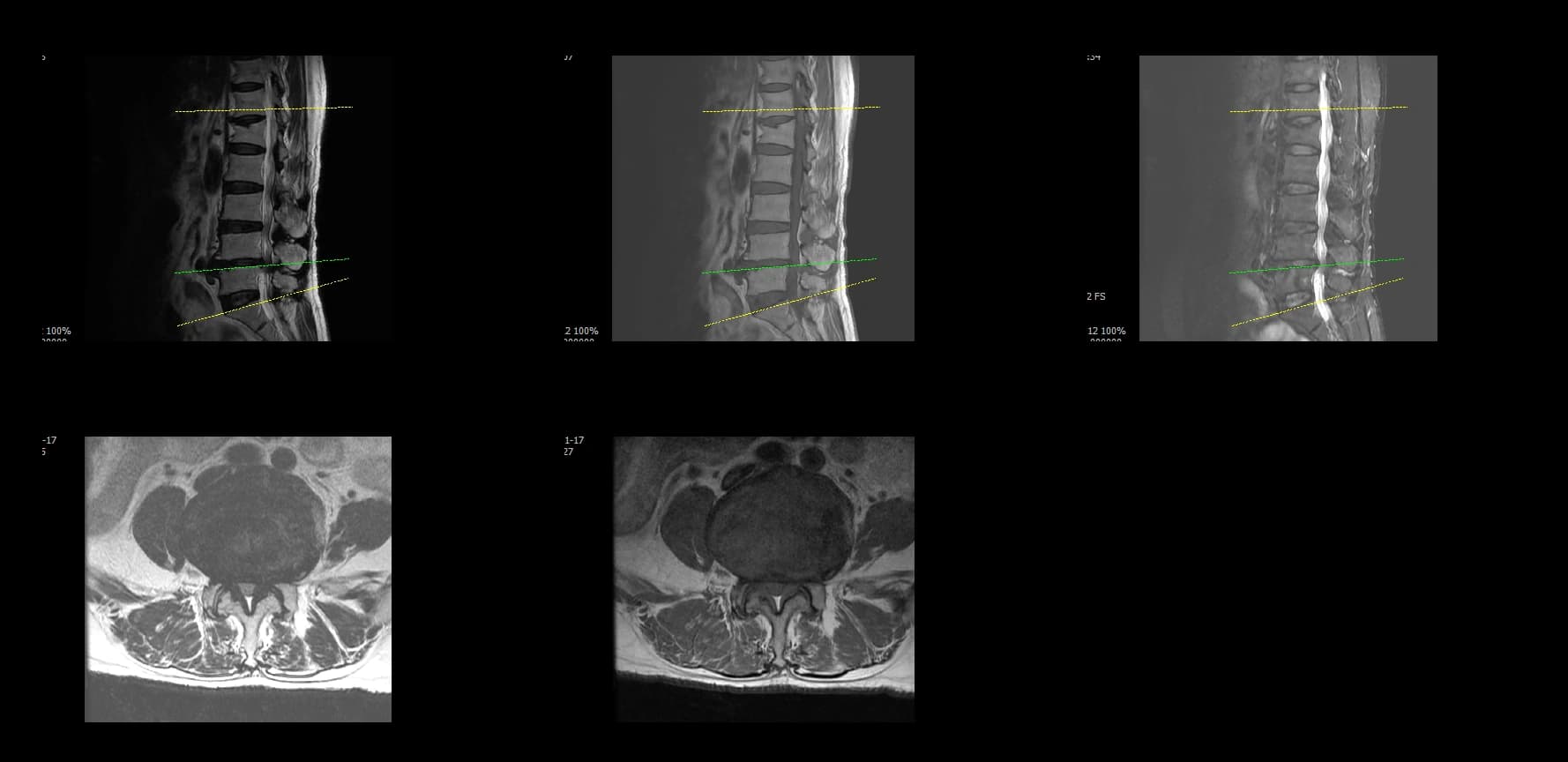
- Imaging summary
- Preoperative lumbar radiographs and MRI demonstrated severe lumbar spinal stenosis at the clinically concordant level or levels. The stenosis pattern included narrowing of the neural canal and compression of the symptomatic neural structures. Imaging findings were interpreted together with the patient's symptoms and neurologic examination rather than as an imaging finding alone.
- Surgical rationale
- Biportal endoscopic decompression was selected to address the symptomatic neural compression while preserving stabilizing structures as appropriate. The surgical target was defined by the relationship between the patient's radicular symptoms, neurologic deficit, and imaging-symptom concordance.
- Operative note summary
- Biportal endoscopic lumbar decompression was performed. The operative workflow focused on identifying the stenotic segment, creating a controlled working corridor, and decompressing the neural elements. A key technical step was careful separation of the adherent ligamentum flavum from the dura. The dissection plane between the hypertrophied or adherent ligamentum flavum and the dura was handled cautiously to reduce dural injury risk during decompression.
- Operative time
- 30 minutes.
- Estimated blood loss
- To be added after de-identification and editorial review.
- Hospital stay
- To be added after de-identification and editorial review.
- Complications
- To be added after de-identification and editorial review. If no perioperative complication was documented, this field may state that no perioperative complication was documented in this educational case summary.
- Postoperative course
- To be added after de-identification and editorial review. If neurologic or symptom improvement was documented, describe it as an observed course in this de-identified case only, not as a promised outcome.
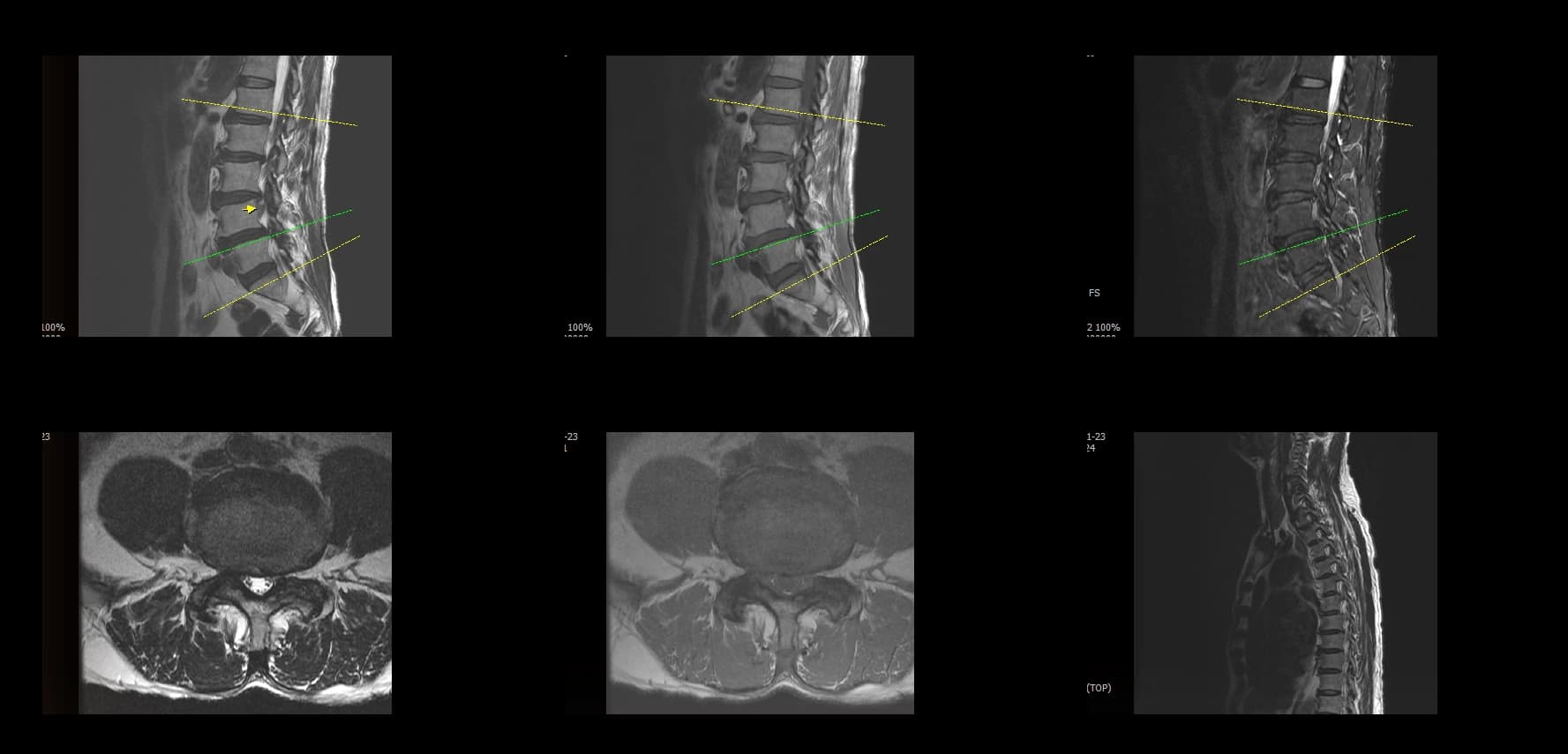
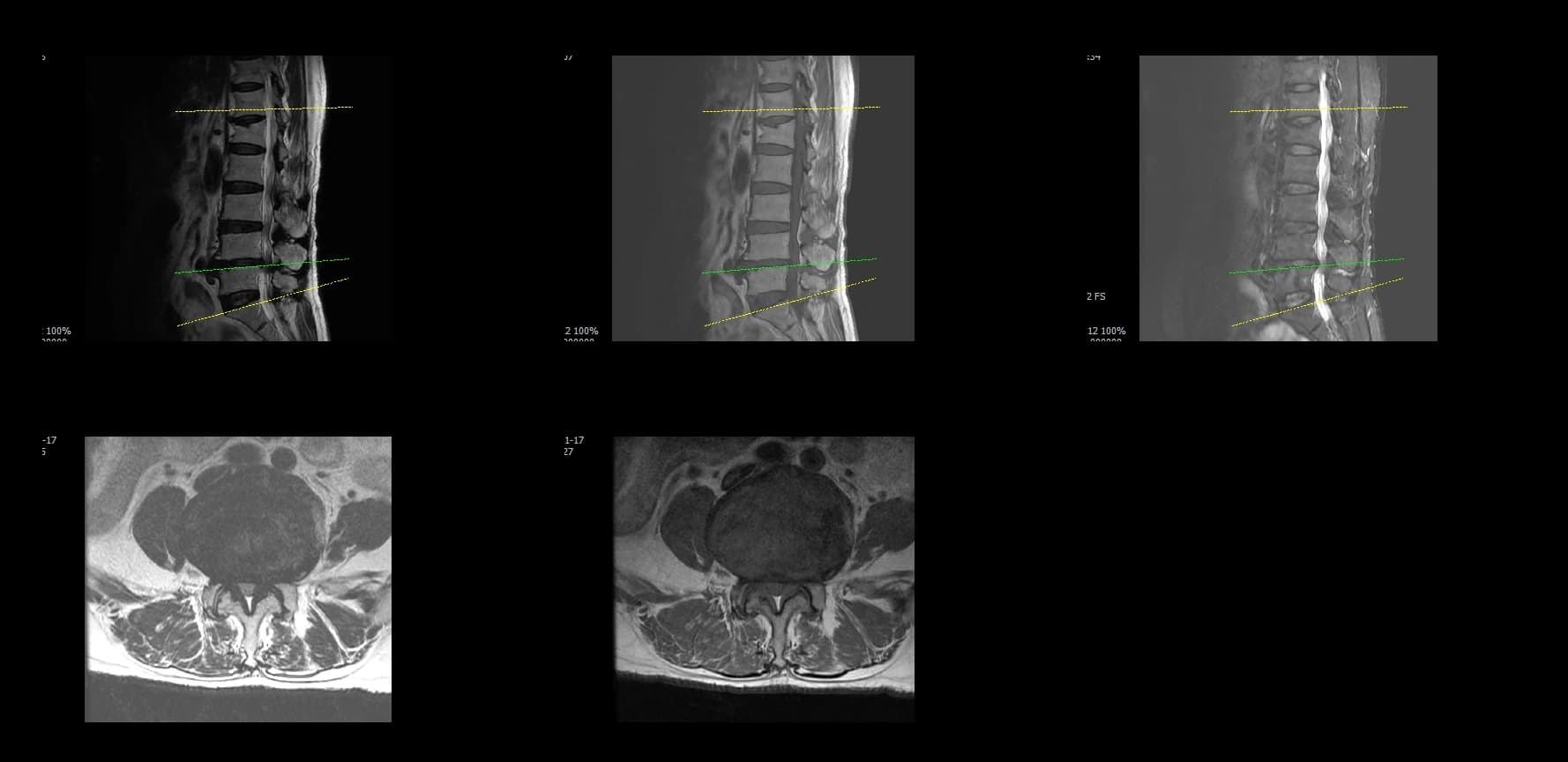
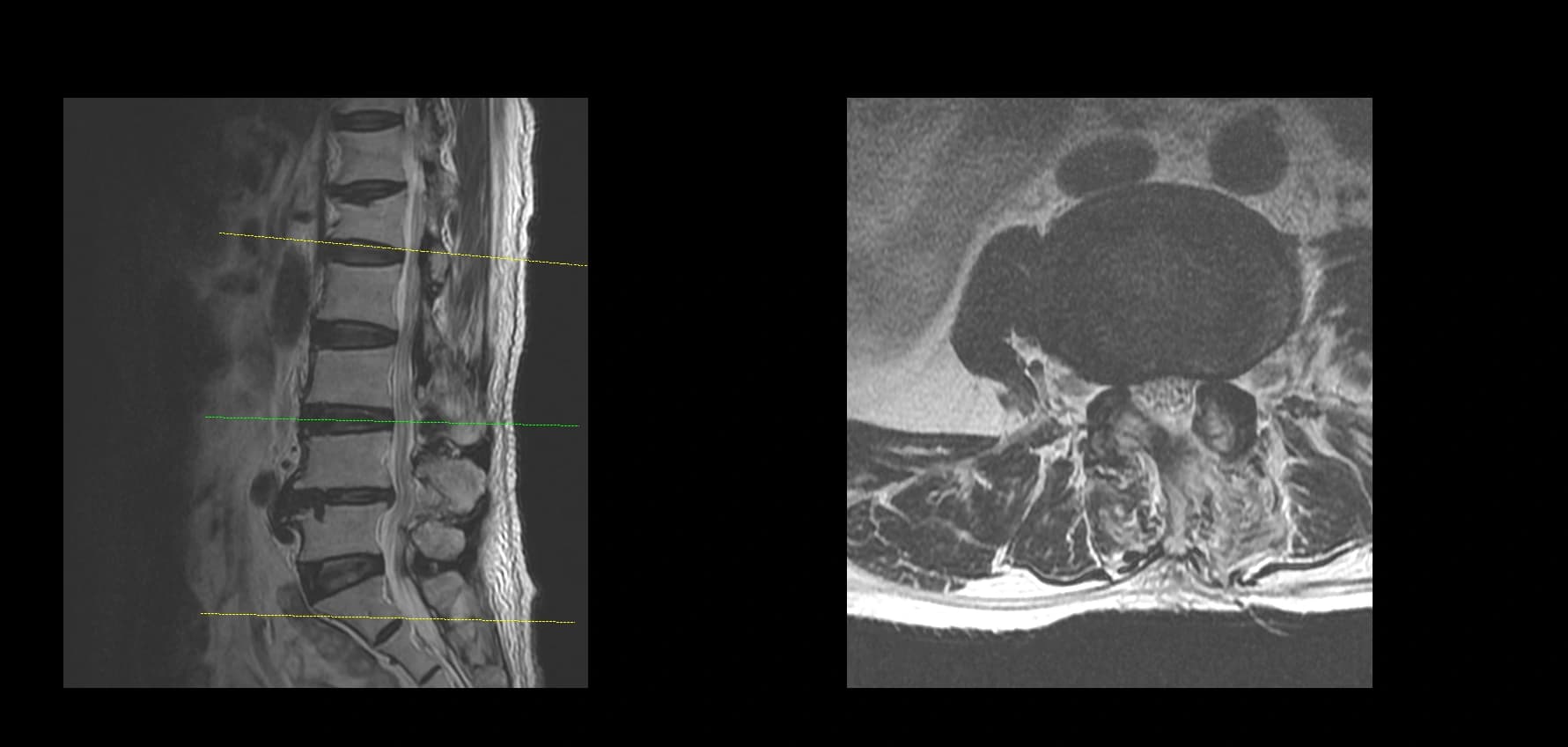
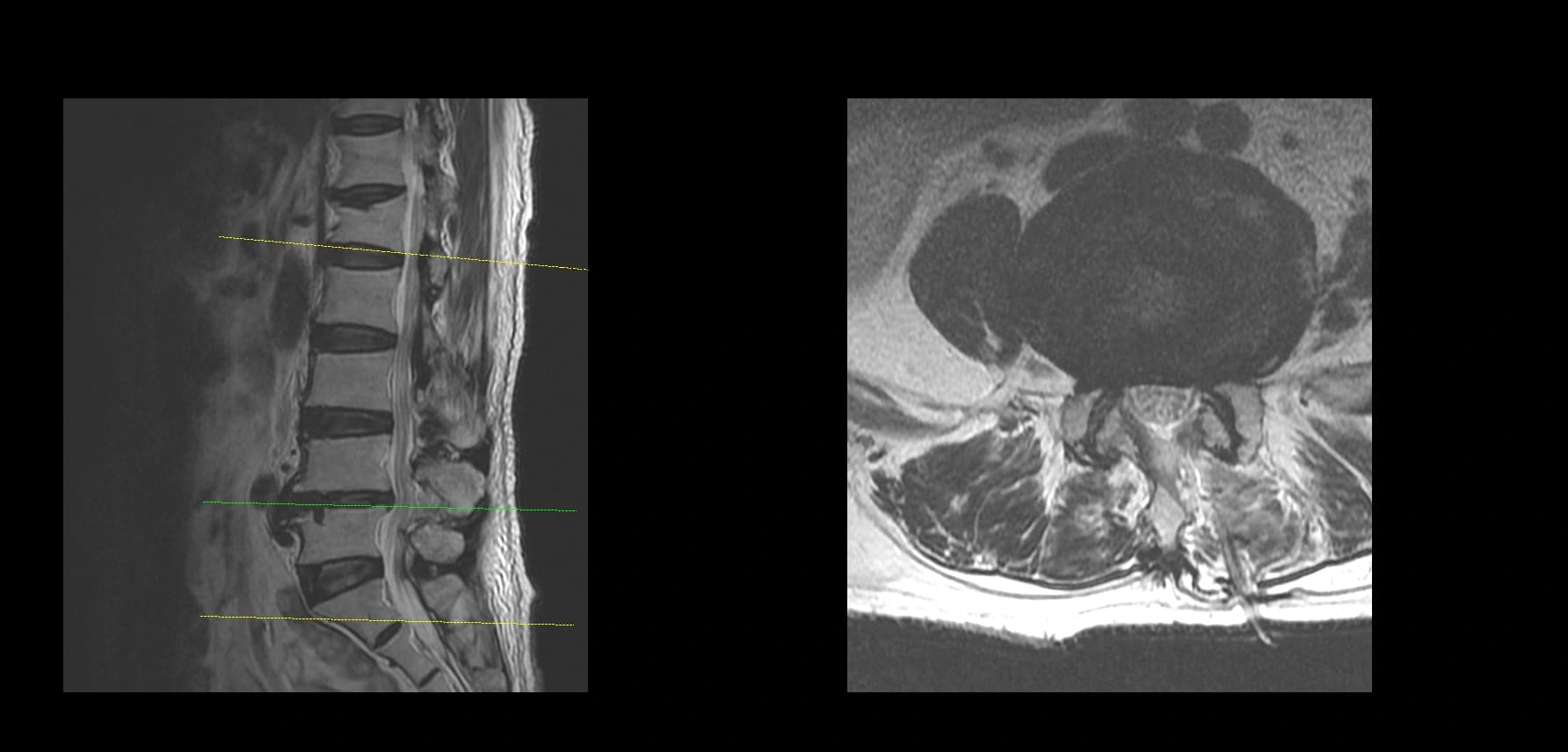
- Postoperative imaging summary
- Postoperative imaging, if used, should demonstrate decompression at the operated level only after full de-identification. Do not include original screenshot overlays or identifiable image labels.
- Educational point
- This case illustrates that severe lumbar stenosis requires precise decompression planning and careful tissue-plane recognition. In severe stenosis, the ligamentum flavum may be hypertrophied or adherent to the dura. Safe decompression depends on identifying and maintaining the correct dissection plane between the ligamentum flavum and the dura, while avoiding unnecessary neural traction or blind instrument movement.
De-identified Clinical Images
Preoperative Images

Postoperative Images
This case is presented for educational discussion only. It is de-identified and should not be interpreted as predicting a similar clinical course in another patient.